The Royal Brisbane Women’s Hospital (RBWH) engaged CSDS to deliver a simulation event for their after-hours Medical Emergency Response Team (MERT) up-late team training program.
The simulation event was based on an elderly male that presents as an agitated, confused patient, who whilst in his distressed state, proceeds to pull out his jugular transvenous pacing wire and develops a 3rd degree heart block.
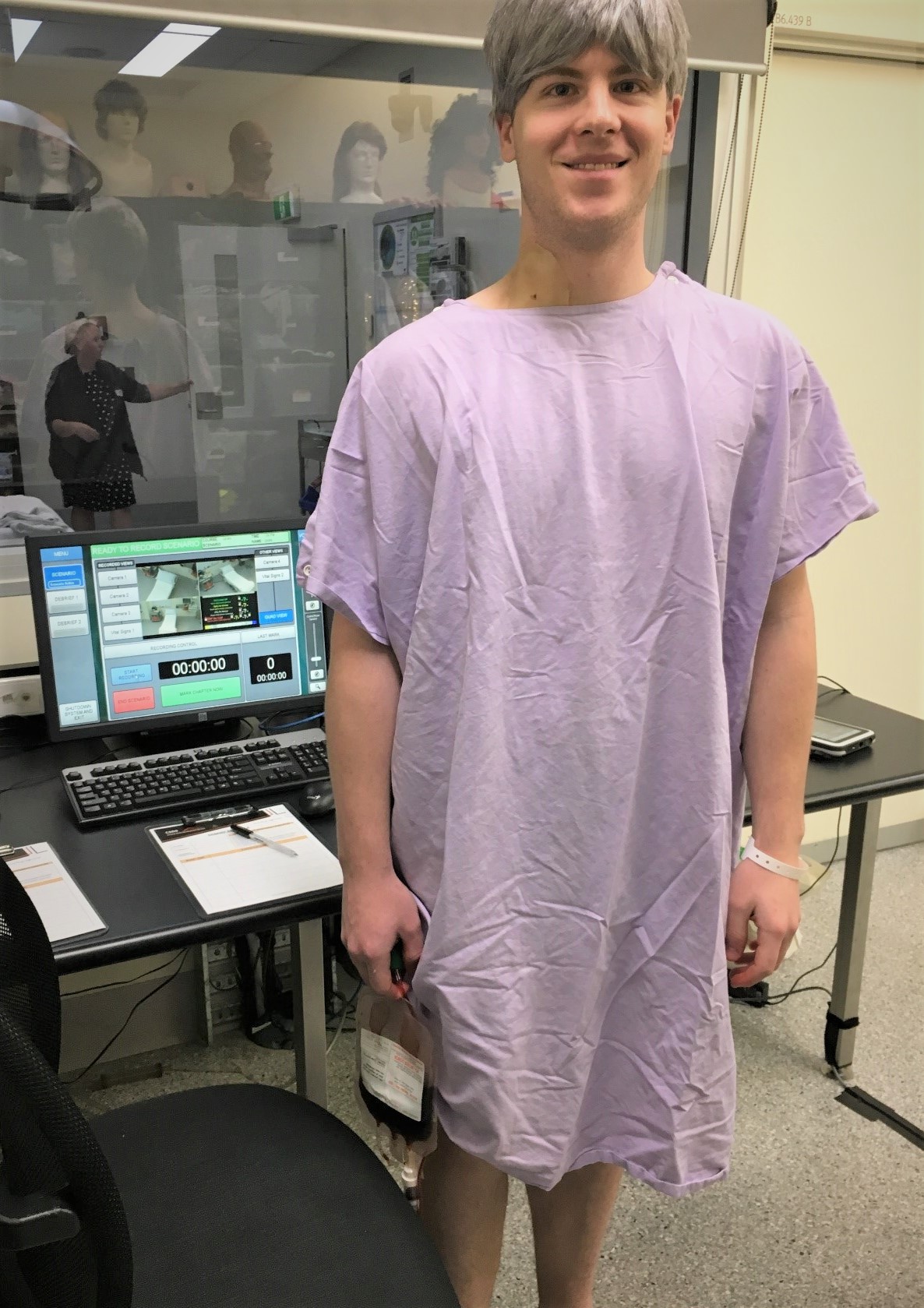
The complex nature of the event required the use of a standardised patient to maintain the immersion and be able to create the right environment for the emergency team to react in the appropriate way. Maintaining immersion is often easier with a live person however does present its own set of challenges.
The big questions for the team became:
- How can we show the bleeding jugular and hematoma?
- More importantly, how can we get the participants to practice external cardiac pacing on a healthy standardised patient?
The team decided to tackle the easiest of the questions first.
How to create a bleeding jugular and hematoma
To solve this issue the team created a neck prosthetic, using a pressure bulb hidden under the patient’s gown, to create the effect of excessive bleeding an IV line is tunnelled under the prosthetic.

To create the prosthetic:
- A two-part Dragon Skin silicone was used with a prepared mould.
- Superglue used to attach the IV tubing underneath the prosthetic.
- Apply the prosthetic to the skin using a safe adhesive, we use Skin Tite bio adhesive to create a strong hold that can withstand the liquid (blood) and not fall off.
- Once securely attached and the adhesive is dry, apply makeup and blend the prosthetic in with the skin to create a more realistic appearance.
The pacing issue was a little bit more complicated.
How to create a cardiac pace on a healthy standardised patient
We have a few options that allow for external cardiac pacing training, including Laerdal Shock-link, and regular manikin operation, as well as the vitalism. The problem remains that none of these are designed for use with a standardised patient.
To bypass this issue:
- Connect a manikin to the Lifepack15 Defibrillator so that the participants would be able to see the 3rd degree heart block display on the defib, as well as be able to pace and see electronic capture.
- Remove the arms and legs from an ALS Simulator Advanced manikin and place it in the tray under the resus trolley.
- Apply the limb leads and defib paddles to the manikin under the bed, tape the cables down and cover the bottom of the trolley with a sheet.
- Tape “dummy” leads and paddle cables to the outlets of the defibrillator to look like they are normal leads and paddles. This allows the participants to perform as normal.
The scenario
Prior to the event the team takes the time to explain the complex setup to the RBWH faculty to prepare them for the situation. Once the team was fully briefed on the scenario details it was time to begin and the participants where sent in.
As the participants begin to walk in the room, the standardised patient immediately proceeds to behave confused and agitated and quickly pulls out his jugular pacing wire. With this the blood comes pouring out of the prosthetic and the first clinician jumped forward and applied direct pressure to the neck. With all the commotion going on the participants didn’t seem to notice the defibrillator cables taped back and the external cardiac pacing went off without a hitch.
There is usually nothing better than having a real person acting as a patient for scenarios that involve managing difficult patient behaviour, and the workarounds really seemed to help the participants buy in.
The event was very successful, and it was brilliant to see how immersed the participants were in the scenario.
If you have any questions about the scenario or any of the materials or tools used please get in contact with us.
Written by Matthys Van Lille, Simulation Co-ordinator at CSDS.